 Research conducted in Sydney, Australia has clarified what has been suspected by a growing number of researchers around the world as major contributors to the cause of plantar fasciitis (heel pain). The research identified that limited ankle range, reduced foot (toe flexor) and leg strength (peroneal strength) and increased bodyweight appear to play a significant role in this condition (Barnes et al., 2017). The study conducted at Sydney University involved several leaders in musculoskeletal research. The research was significant for both the quality as well as the breadth of the research that was conducted. The study compared 71 people with long term heel pain with 61 people who had heel pain of less than 6 months. This world leading research group used this 2017 publication to extend on the research they published in 2015 in which 202 people with heel pain were compared with 70 well matched controls. Both papers evaluated an extensive range of factors (outlined below) to isolate which of these appear to be the most important in clinical assessment and treatment. The factors evaluated have at various times been implicated in the development of heel pain but required further research. The factors included: Biomechanical alignment; joint mobility; muscle strength of both the foot and leg; calf endurance; and weightbearing activity levels. Importantly this research has clarified what is not likely to be important in plantar fasciitis. Specifically heel pain was not associated with big toe range of motion (either high or low flexibility); excessive flexibility of the arch (hypermobility); calf strength or calf endurance; inwards or outwards movement of the foot; foot alignment; occupational standing time, or exercise level. Interestingly it has shined a light on the work of Rathleff et al. in 2009 which appeared to indicate that high load strength training for the calf muscles was an effective treatment for plantar fasciitis. The new research from Barnes proved this unlikely to be the case indicating both calf strength and endurance were not associated with heel pain risk. The research by Rathleff has been criticised previously. Specifically, it was criticised for its methodology which a) combined multiple treatments at once but singled out high load calf strengthening as the over-riding effective treatment b) had no control group and c) showed that strengthening took a very long time to take effect in respect to normal clinical practice i.e. 3 months and d) the groups were only different at the 3 month point and in fact the strength group were slightly, but not statistically significant, worse at the end of the study than the non-strength group (Rathleff et al., 2015). Only the non-strengthening group had subjects who reported no pain at the 12-month point. Interestingly, the natural history of plantar fasciitis even without treatment has been suggested to be 12 months (Caselli et al., 1997). 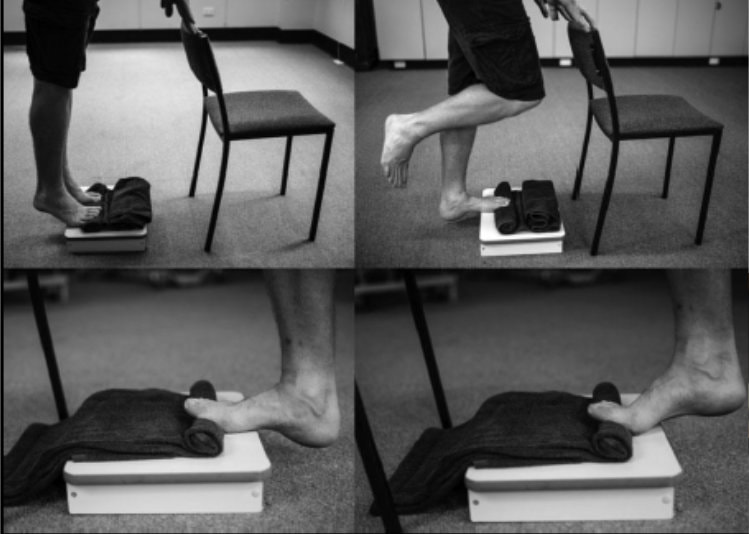 However, there are important aspects to the Rathleff study. The calf exercises in the study are done through a full range and involve eccentric loading. This is likely to be an effective way of maximising flexibility of the ankle, in keeping with the new research paper which suggested that reduced ankle range may be of significance as a cause of plantar fasciitis. Eccentric loading in a lengthened position is also likely to result in the addition of sarcomeres in series (sarcomerogenesis) to the calf muscle improving its resting length and therefore improving ankle range. These adaptations also potentially increases the joint angle at which peak torque is generated (O’Sullivan, McAuliffe and DeBurca, 2012). All of this is likely to improve better ankle control through its entire range, improve better control of forward body movement (especially in the case of increased BMI) and ultimately helps to unload the plantar fascia through the propulsive period of gait. Thus, asking patients to perform calf strengthening exercises on a step is likely to be helpful, especially through the full lower range, although we are unsure as to whether placing a towel under the toes whilst doing this is necessary. About heel pain Plantar heel pain is the most common foot disorder treated by health care practitioners (Martin et al., 2014). It occurs mainly in adults and effects people who come from both active and sedentary lifestyles. In the United States approximately 2 million people seek treatment for plantar heel pain every year, at a cost of more than $300 million (Riddle and Schappert, 2004; Tong and Furia, 2010). Heel pain is believed to occur due to excessive cumulative strain at the attachment of the plantar fascia and mechanical overload is thought to play a major role in causing this condition. Best care of heel pain has alluded practitioners for decades with researchers in the past being unable to identify the likely causative factors. References Barnes, A. et al. (2017) ‘Clinical and Functional Characteristics of People With Chronic and Recent-Onset Plantar Heel Pain’, PM and R. American Academy of Physical Medicine and Rehabilitation, 9(11), pp. 1128–1134. doi: 10.1016/j.pmrj.2017.04.009. Caselli, M. et al. (1997) ‘Evaluation of magnetic foil and PPT Insoles in the treatment of heel pain’, Journal of the American Podiatric Medical Association, 87(1), pp. 11–16. doi: 10.7547/87507315-87-1-11. Martin, R. L. et al. (2014) ‘Heel Pain—Plantar Fasciitis: Revision 2014’, Journal of Orthopaedic & Sports Physical Therapy, 44(11), pp. A1–A33. doi: 10.2519/jospt.2014.0303. O’Sullivan, K., McAuliffe, S. and DeBurca, N. (2012) ‘The effects of eccentric training on lower limb flexibility: A systematic review’, British Journal of Sports Medicine, 46(12), pp. 838–845. doi: 10.1136/bjsports-2011-090835. Rathleff, M. S. et al. (2015) ‘High-load strength training improves outcome in patients with plantar fasciitis: A randomized controlled trial with 12-month follow-up’, Scandinavian Journal of Medicine & Science in Sports, 25(3), pp. e292–e300. doi: 10.1111/sms.12313. Riddle, D. L. and Schappert, S. M. (2004) ‘Volume of Ambulatory Care Visits and Patterns of Care for Patients Diagnosed with Plantar Fasciitis: A National Study of Medical Doctors’, Foot & Ankle International, 25(5), pp. 303–310. doi: 10.1177/107110070402500505. Tong, K. B. and Furia, J. (2010) ‘Economic burden of plantar fasciitis treatment in the United States’, American Journal of Orthopedics (Chatham, Nj), 39(5), pp. 227–231.
4 Comments
17/4/2023 12:42:18 pm
Thank you for pointing out that further study was needed to determine the causes of heel discomfort, which included biomechanical alignment, joint mobility, muscular strength in the foot and leg, calf endurance, and degrees of weight-bearing exercise. My friend is employed by a building company. He laments the ache in his heel. I'll advise him to consult an expert to determine the proper cause of his heel discomfort. 18/11/2023 12:14:07 pm
What is the varicose vein that usually appears on women in the world and comes across as a disease? What are the symptoms of varicose veins? https://turkeymedicals.com/esthetic/vein 23/11/2023 07:30:25 pm
What is Genome Sequencing? 30/11/2023 12:10:11 am
Invoice Review: You should check the accuracy by reviewing the invoice sent to you. If there is an inaccuracy or incorrect information, you can request a correction by contacting the hospital authorities. Leave a Reply. |
AuthorMatt Dilnot is a Podiatrist working in the Eastern Suburbs of Melbourne, Victoria. Archives
May 2020
Categories
All

|
 RSS Feed
RSS Feed