|
Let’s cut to the chase - if you have an ankle equinus (lack of ankle dorsiflexion) it means that you have an increased chance of developing retracted toes. The greater the equinus the more chance your toes will retract upwards (Cheuy et al., 2015). 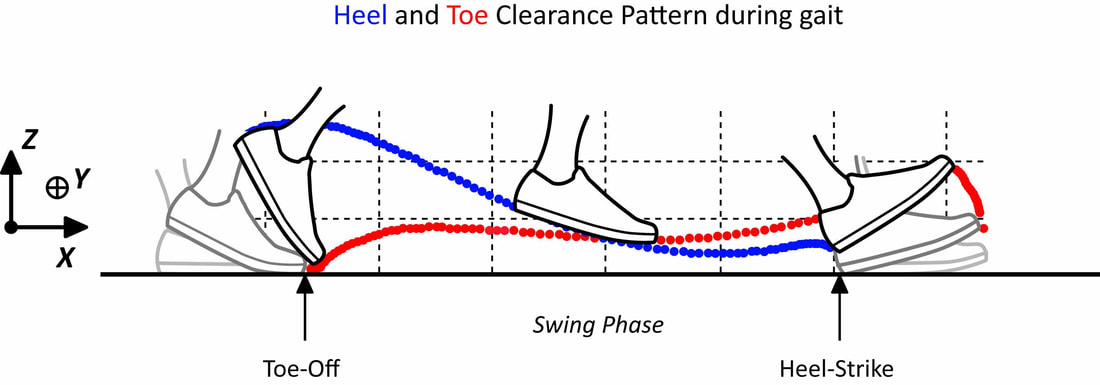 Your toes retract upwards through increased activity of the extensor muscles (extensor digitorum/hallucis longus/brevis) in response to the restriction in ankle range (most likely due to a short calf). Luckily these extensor muscles do work harder otherwise people with reduced ankle range would trip over their toes during the swing phase of gait. Ground clearance during swing phase is not very large (less than 2 cms for most people depending on height) (Winter, 1992). The downside of the increased extensor activity is it causes greater and greater hyperextension of the MTPJs and makes it harder for the intrinsics to keep the toes straight. During propulsion the lumbricals and interossei become ineffective in stabilising the toes and all we have left are the extrinsic flexors (Flexor digitorum longus which causes the toes to claw without the work of the intrinsics). Therefore, to stop this process we can’t just focus on intrinsic muscle strengthening. The fault in many cases can be the reduced range at the ankle joint (especially in diabetes). For the most part, patients with this limitation primarily have calf weakness and subsequent shortening (they go hand in hand e.g. if you immobilize the calf, it weakens and shortens itself to maintain a healthy length-tension relationship) (DiGiovanni et al., 2002). In diabetes the restriction is in combination with AGE’s (Advanced Glycation End products) which essentially decreased the flexibility of collagen (Rao et al., 2006). To get the best and most effective result for our patients we need to ask them to strengthen their calf muscles by performing an eccentric calf loading program. Eccentric strengthening of muscles in a lengthened position promotes greater strength and length by promoting the physiological process of sarcomerogenesis (Lynn and Morgan, 1994), essentially a process by which the muscle makes itself longer by adding on sarcomeres in series. Once you have done exercise in this way for a few months you will end up with an increased muscle resting length which will return some if not all the lost range in the ankle joint. In doing so you have reduced the need for the extensor muscles to work so hard to clear the ground. In return the patient will have improved range and power in propulsion which will have added benefits for hip and knee function. This is also by far a more effective program than stretching the calf muscles which will only offer short term benefits. Essentially using the ToePro to perform calf eccentric exercises combined with the intrinsic strengthening aspect will give patients a very effective approach to maximising their potential to improve range and improve toe alignment and strength. When do we call it quits? The problem that will raise its head very quickly for patients is that if they have walked in this way for a long period of time the flexion deformity they have developed in their toes may have become fixed. The calf exercises will still be effective in improving the ankle range if the equinus is due to the tightened calf muscles. It will also reduce the risk of further progression of the deformity and should therefore be recommended and most likely will benefit more proximal joints. It would not be unreasonable to recommend stretching of the shortened extensors passively (by say the hands, or by sitting on top of your feet with your feet maximally plantarflexed beneath you) or even to recommend strengthening the extensor tendons in a lengthened position also. The practitioner can also perform mobilisation and manipulation of both the ankle and toes to improve their range. References Cheuy, V. A. et al. (2015) ‘Muscle and Joint Factors Associated with Forefoot Deformity in the Diabetic Neuropathic Foot’, Foot and Ankle International, 37(5), pp. 514–521. doi: 10.1177/1071100715621544. DiGiovanni, C. W. et al. (2002) ‘Isolated gastrocnemius tightness’, Journal of Bone and Joint Surgery - Series A, 84(6), pp. 962–970. doi: 10.2106/00004623-200206000-00010. Lynn, R. and Morgan, D. L. (1994) ‘Decline running produces more sarcomeres in rat vastus intermedius muscle fibers than does incline running.’, Journal of applied physiology (Bethesda, Md. : 1985), 77(3), pp. 1439–1444. doi: 10.1152/jappl.1994.77.3.1439. Rao, S. R. et al. (2006) ‘Increased passive ankle stiffness and reduced dorsiflexion range of motion in individuals with diabetes mellitus’, Foot and Ankle International, 27(8), pp. 617–622. doi: 10.1177/107110070602700809. Winter, D. A. (1992) ‘Foot Trajectory in Human Gait: A Precise and Multifactorial Motor Control Task’, Physical Therapy. Oxford University Press, 72(1), pp. 45–53. doi: 10.1093/ptj/72.1.45.
2 Comments
15/5/2023 01:10:35 pm
Thank you for the helpful information. If you want to know more about foot problems, treatment and others, you can visit this site. Leave a Reply. |
AuthorMatt Dilnot is a Podiatrist working in the Eastern Suburbs of Melbourne, Victoria. Archives
May 2020
Categories
All

|
 RSS Feed
RSS Feed